'%3e%3ctitle%3ehospital%3c/title%3e%3cpath d='M9.6 4c-0.896 0-1.6 0.704-1.6 1.6v6.4h-6.4c-0.896 0-1.6 0.704-1.6 1.6v4.8c0 0.896 0.704 1.6 1.6 1.6h6.4v6.4c0 0.896 0.704 1.6 1.6 1.6h4.8c0.896 0 1.6-0.704 1.6-1.6v-6.4h6.4c0.896 0 1.6-0.704 1.6-1.6v-4.8c0-0.896-0.704-1.6-1.6-1.6h-6.4v-6.4c0-0.896-0.704-1.6-1.6-1.6z'/%3e%3c/svg%3e)
- MEDICAL SERVICES (PVT) LTD.

Theoretical background of the mission
(සේවාවන්හි සිද්ධාන්තික පසුබිම - සිංහල පරිවර්ථනය වෙබ් පිටුවෙහි පහලින්)
This new health care service business entity involves few other fields in addition to the field of medicine. These fields include management science, information technology & co-operative movement principles. In the explanation of theoretical background of this mission the theory behind each field is briefed and the operational concepts of each theoretical part are highlighted below.
1. Theoretical background of medical science concepts
This mission is almost totally targeted towards the non-communicable (non-infectious) diseases (NCDs), preventive medicine, health promotion & individual health management.
1.1 Non communicable diseases
Non communicable diseases are defined as a medical conditions or diseases that are non-infectious or non-transmissible. NCDs can refer to chronic diseases which last for long periods of time and progress slowly. Sometimes, NCDs result in rapid deaths. While sometimes (incorrectly) referred to as synonymous with "chronic diseases", NCDs are distinguished only by their non-infectious cause, not necessarily by their duration. Some chronic diseases of long duration, such as HIV/AIDS, are caused by infections. Examples for these diseases are, diabetes mellitus, cancers, heart diseases, blood cholesterol or lipid abnormalities, stroke, autoimmune diseases, cancers, chronic kidney disease, osteoporosis, Alzheimer's disease, etc. These are preventable diseases.
1.2 Preventive medicine
Preventive medicine is defined as medical techniques and treatments intended to prevent disease before it happens, rather than curing it.
1.2.1 Basic principles of preventive medicine are.
- Primary prevention - Methods to avoid occurrence of disease by health promotion efforts.
- Secondary prevention - Methods to diagnose & treat existent diseases in early stages, before it causes significant morbidity.
- Tertiary prevention - Methods to reduce negative impact of existent disease by restoring function & reducing disease related complications.
- Quaternary prevention – Method to mitigate or avoid results of unnecessary or excessive interventions in the health care system.
1.2.2 Explanation
Although there are a wide variety of interventions that may reduce the actual occurrence of a disease or disorder and thus in the most general sense are "preventive," not all of these efforts are appropriately labeled as prevention. Primary prevention should be accorded its own unique status, and secondary prevention given the more descriptive and appropriate label of early intervention. Similarly, treatment also should be accorded the separate and unique status it requires, rather than simply being lumped as merely another form of prevention. The unique and defining features of prevention programs are (1) in their timing, (2) the levels of analysis that are targeted, and (3) the conditions that are the direct or indirect targets of change. Given the "before-the-fact" nature of primary prevention, it could be argued that any intervention to reduce a specific behavior targeted at a group of individuals who have not yet demonstrated the behavior would qualify as prevention. Here the reasoning is that because they have not yet acted in a problematic way, they do not yet have the disorder. However, it is difficult to identify the specific point of "onset" for many socioemotional and health-related disorders.
A second critical feature of prevention programs relates to the level of analysis to which they are subjected. Prevention initiatives are targeted to populations or subpopulations, and the individuals who are the recipients of the intervention are selected based on their membership in the target group, rather than through a process of screening and selection based on individually specific characteristics. Once interventions move to such screening and identification of conditions that are specific to discrete individuals, they have moved to early intervention and/or treatment. The targeting of populations is based on their exposure to conditions of risk (which are always population or subpopulation-level, never individual-level conditions) or the lack of exposure to important protective and developmentally enhancing conditions.
The third defining feature for prevention efforts relates to what is targeted. In early intervention or treatment, there are clearly identifiable, highly individually specific conditions that need to be reversed or strengthened. These conditions are the direct targets of change and the evaluation of programming can follow from them, in that changes in these focal conditions will be apparent. In prevention, the first and second-order targets of change are those conditions that lead to the focal conditions. First-order targets of change, or those conditions that are most directly targeted for change by the intervention, are the conditions of risk or protective factors to which all members of the population or subpopulation are exposed that have been identified as etiologically significant. Second-order targets of change are the levels of those vulnerabilities and competencies that result from exposure to the risk and protective factors of concern. Finally, through the modification of these critical elements of the etiological pathway, the incidence and prevalence of the targeted disorder or dysfunction will be affected. Prevention applies to the systematic enhancement, disruption, alteration, or modification of the developmental processes (and conditions) that lead to well-being or to serious mental illness or social problems.
The major evolutions in related fields are:
1. Epidemiology-the definition and classification of disease processes; the identification and elaboration of risk factors; the modeling of causal relationships between and among risk and demographic variables; the accurate measurement and reporting of behavior in a defined population over time (surveillance)
2. Treatment-the evolution of techniques and technologies to effectively and efficiently treat individuals demonstrating early (and sometimes late) the signs and symptoms of distress and disorder.
3. Community mental health movement-a recognition of the power and importance of the role of family community, schools, and workplace on the etiology, maintenance, and exacerbation of individual and group disturbance; the recognition of the powerful roles of ecology and environment in the development, expression, and maintenance of disordered social systems that express themselves as beliefs, attitudes, and behavior.
1.3 Health promotion
Health promotion is defined as the process of enabling people to increase control over, and to improve, their health to reach a state of complete physical, mental and social well-being. An individual or group must be able to identify and to realize aspirations, to satisfy needs, and to change or cope with the environment. Health promotion is, therefore, seen as a resource for everyday life, not the objective of living.
Health promotion is a positive concept emphasizing social and personal resources, as well as physical capacities. Therefore, health promotion is not just the responsibility of the health sector, but goes beyond healthy life-styles to well-being.
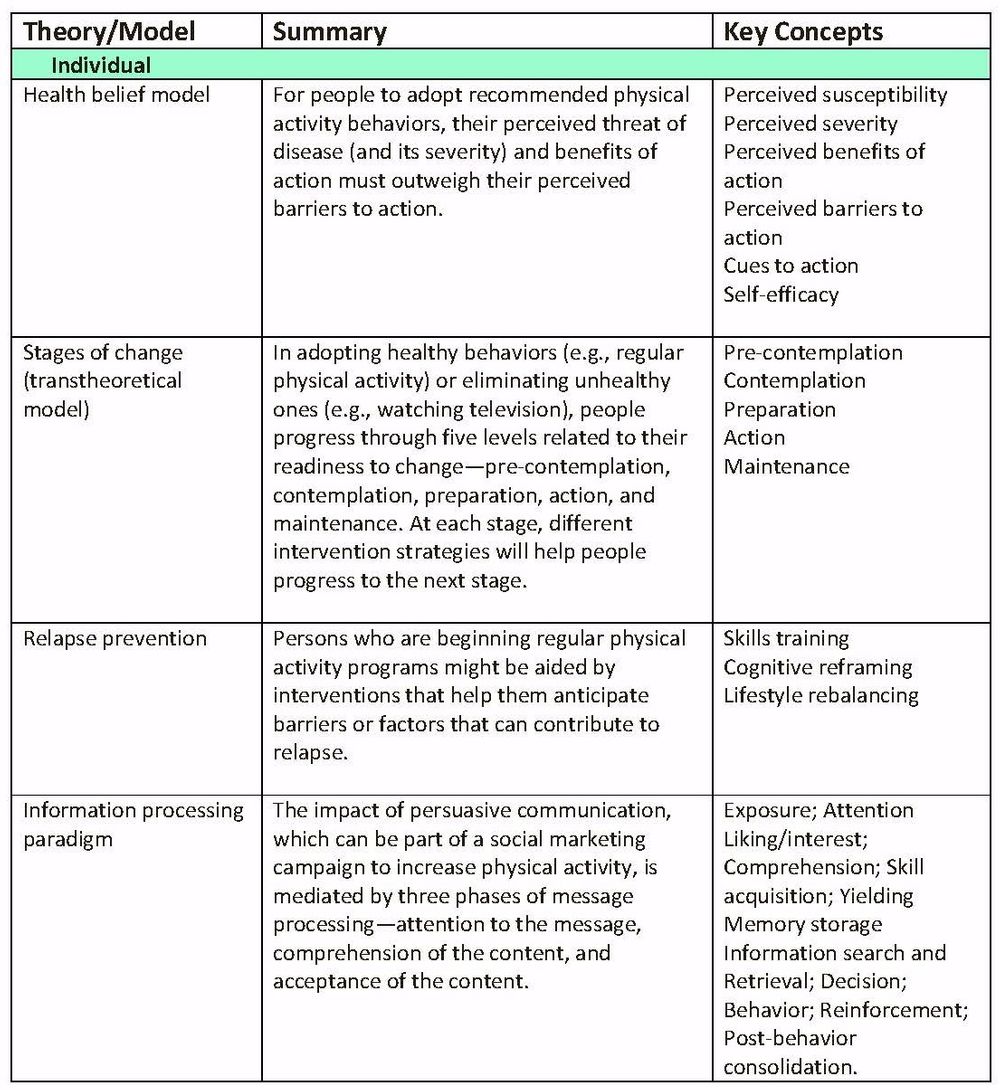
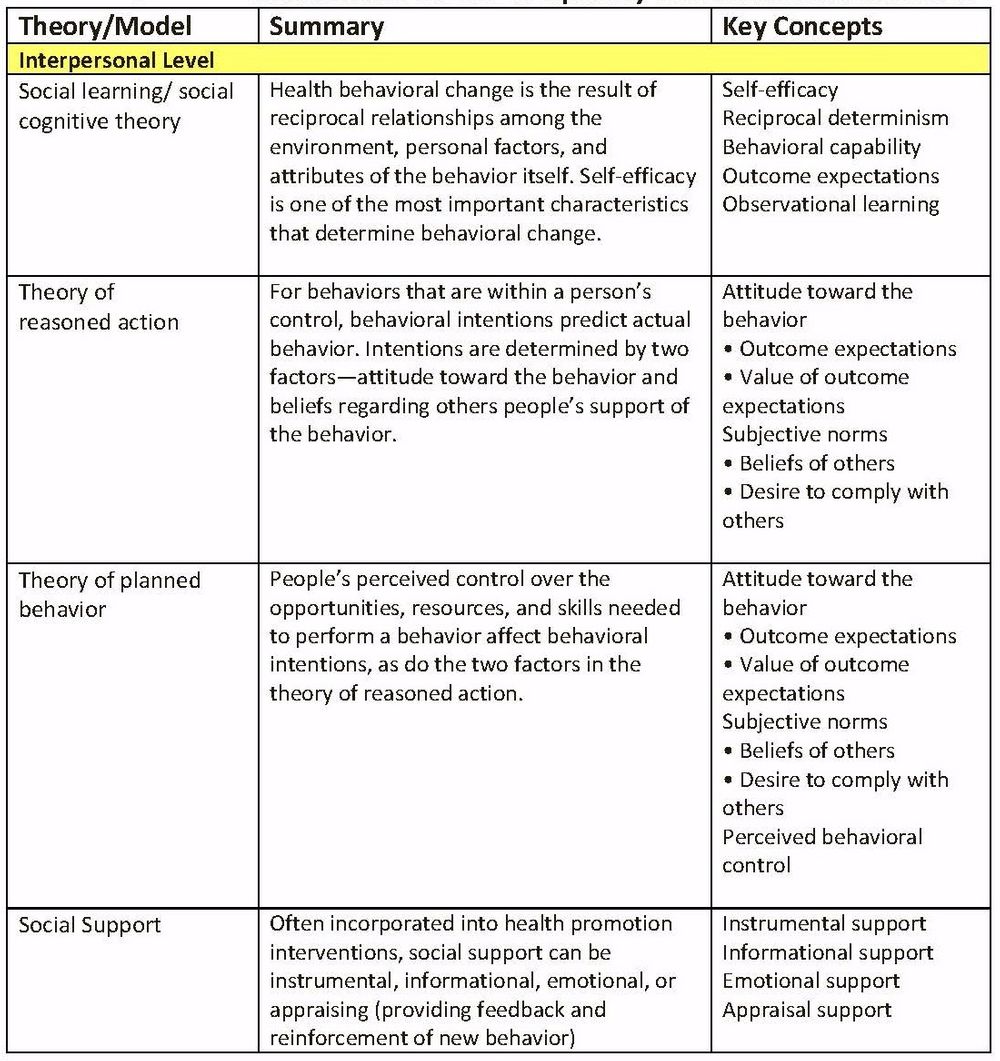
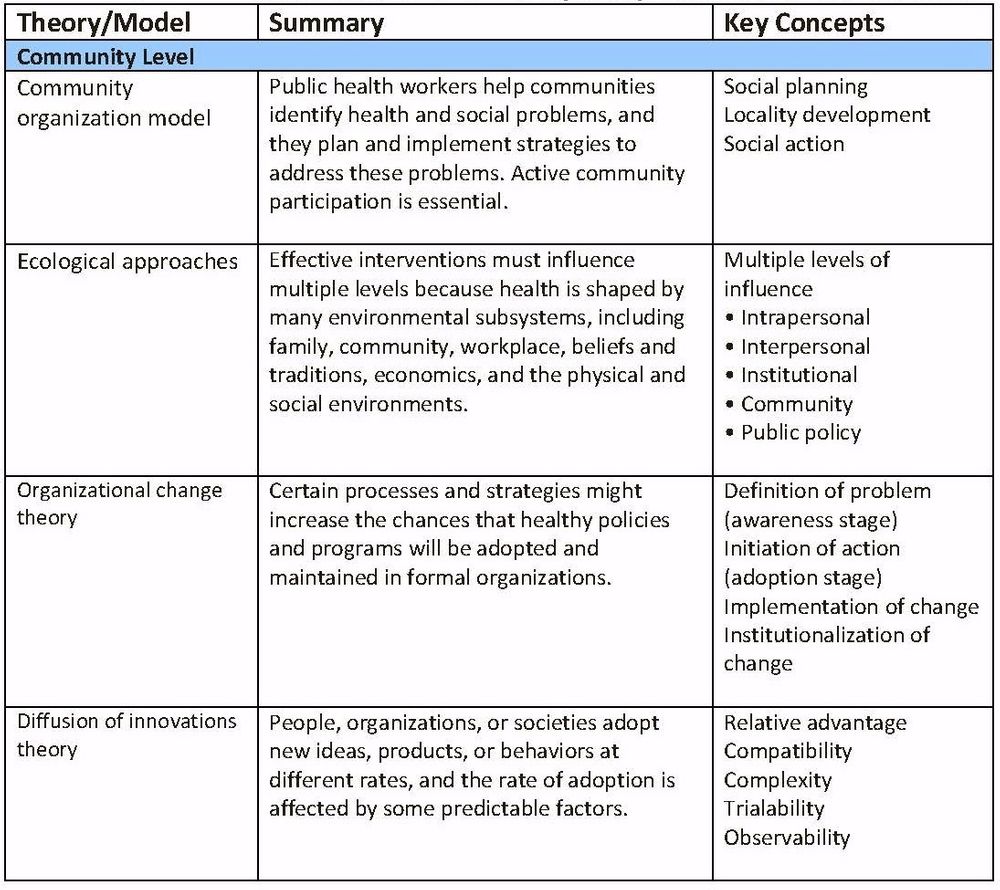
1.3.1 Theories and models frequently used in health promotion
1.4 Health management
It is important to look at the definition of health and then health care before looking at the definition of health care management. World Health Organization (1948) defined health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”. It assesses the totality of someone’s mind and body. Health care in itself may be defined as the act of restoring and maintenance of the health of people by the prevention and treatment of diseases by health professionals who are trained and licensed in the field.
Health care management according to Jones & Bartlett (2011) is defined as “the profession that provides leadership and direction to organizations that deliver personal health services and to divisions, departments, units, or services within those organizations”.
Health Care Management can also be defined as one of the following ways.
It refers to the management of hospitals, hospital networks, and/or health care systems, at the different levels of organization and planning of clinical activities and support processes.
It also referred as medical and/or health services or health administration. Health management ensures that the outcomes are attained, that different areas within a health organization are running appropriately, that jobs are correctly defined and assessed and that resources are used efficiently.
It also referred as the act of preventing, treating and managing illness, including the preservation of mental and physical problems through the services provided by health professionals.
Health care organizations are effective and also complicated. For health care organizations to achieve their goals and objectives, the health care managers must be effectively ınvolved ın the process of leadıng, supervisıng and coordinatıng employees because an organization cannot succeed based on the capacity or intelligence of an individual. The managers must ensure that the human and non-human resources of the organization are adequately utilized. Health care managers are in the position of authority to develop the organization by making principal decisions in the areas of recruiting, selecting and developing staffs, acquiring technology, and judicious allocation and spending of financial services. The health care managers are not just to focus on making decisions that will allow patients to receive quality and affordable services, but also to measure and compare their performance targets with respect to their decisions, because any decision made by a health manager could influence the comprehensive achievement of the organization whereas the medical experts, nurses, laboratory technicians and other health care workers provide services to patients; to be able to generate dividend, deliver standard service and sustenance, health care managers must be available. Some of the functions of health care managers include but are not limited to the following:
- · To promote an environment that can yield standard health care services at maximal profit. · Make decisions, coordinate and delegate authorities. · They decide the number of health workers required in a district. · They monitor the quality of drugs in their district · They report the performance of their health district to the government and stakeholders. · They develop and maintain health facilities in their district. · They cooperate with medical and non-medical staffs for the smooth running of the organization. · They make financial forecasting and also monitor health expenses against budgets in the district. · They oversee all the day-to-day activities of the organization.
1.4.1 Historical health management theories.
The reformation of industries along with the development and increase of patient-centered management theory. This approach has been adopted by organizations in changing the behavior towards care of patients and improving health care working conditions. This theory involves designing systems in such a way that ensures optimum health care services are delivered to patients. This is done at the costs of senior managers designing the system in consideration of easier ways to supervise and the cost efficiency. The main aim of this theory is that by excellence in medical services, health care organizations will attain optimum financial results. Collaboration between different departments and interdisciplinary procedures are applied under this approach to solve medical issues.
1.4.2 Health planning is also a part of health management.
According to World Health Organization (2015), “Health planning is the orderly process of defining health problems, identifying unmet needs and surveying the resources to meet them, establishing priority goals that are realistic and feasible, and projecting administrative action, concerned not only with the adequacy, efficacy and efficiency of health services but also with those factors of ecology and of social and individual behavior that affect the health of the individual and community.” It is a process to produce health and its planning process is done by the ministries of health in the government agencies and can also be delegated to different non-government bodies. The health planning process can also be carried out by service providers (private organizations) like private hospitals, pharmaceutical companies and other service providers. Health professional bodies (like Doctors, nurses, to name a few) are also involved in the health planning process where they input issues that are of interest to them. The health planning process involves the following; (a) Surveying the environment (what is) (b) Setting directions (what ought to be) (c) Problems and challenges (differences between what is and what ought to be) (d) Range of solutions. (e) Best solution(s) (preferred ways to get to what ought to be) (f) Implementation (putting in place the best solution) (g) Evaluation (Did we get from what is to what ought to be?).
1.5 What is e-health:
E-health is the use of information and communication technologies (ICT) for health. The sub category “m-health” is the use of mobile wireless technologies for public health. It is a relatively recent healthcare practice dating back to at least 1999. WHO assembly in 2013 recognized the need for health data standardization to be part of e-health systems and services, and the importance of proper governance and operation of health-related internet domains. Leaders and policy makers on a global scale are strongly encouraging the use of e-health technologies. Australia, Europe, South Korea, and the United States all have strong e-Health initiatives that are developing policy for using information technology to improve health and health care systems. The Washington think tank “e-health Initiative” (promoting policy focused on research and education in e-health), the Institute of Medicine (IOM), and the Agency for Healthcare Research and Quality (AHRQ) also recommend the use of e-health as a tool to support self-management in chronic illness. Large systematic reviews conducted by the AHRQ determined that eHealth tools can improve patient engagement and health outcomes; however, more research is needed. Jimison et al [14] also identified that e-health technology interventions must contain a closed or complete feedback loop (CFL) to have an impact on chronic illness outcomes. A complete feedback loop contains five stages: (1) transmission of data and information regarding the health status of the consumer, (2) interpretation of data and information using previously established knowledge and/or wisdom and use of evidence-based standards, (3) address the specific need of the individual consumer, (4) timely feedback to the consumer addressing their requirements, and (5) regular repetition of the feedback loop. Despite the strong push for e-health, there is no standard definition, which hinders research and implementation. Comprehensive systematic reviews have identified as many as 51 different definitions for e-health in the literature. Overall, the literature describes the definition of e-health to be very broad and encompassing, ranging from the very business-oriented to more clinically focused. The Internet serves as a conduit for self-management support, connecting providers and consumers to secure portals, health applications, social networks, and large databases. In developed countries roughly 80% of adults have sought health information on the Internet, including 62% of adults with a chronic illness.
1.6 The definition of e-health for chronic illness self-management:
Promotion of positive health outcomes by using a new frame of mind that incorporates information and communication technologies in the presence of a complete feedback loop and enables the use of data and information, to generate health management knowledge and wisdom.
1.7 What is Chronic Care Model (CCM):
CCM is a well-established and validated framework that illustrates a comprehensive approach to caring for the chronically ill that supports increased functional and clinical outcomes. The model includes six key interdependent components: (1) community resources, (2) health system support, (3) self-management support, (4) delivery system design, (5) decision support, and (6) clinical information systems. The Chronic Care Model was initially developed by the MacColl Institute USA. The CCM places chronic care in the context of the community where the person will receive health care services and with the health systems involved in that care. The CCM highlights the importance of “Self-Management Support”, giving patients the knowledge, confidence, and skills for self-management of their condition. “Delivery System Design” is also important to promote a patient-centered interdisciplinary team approach to care. “Decision Support” is needed to assure providers and patients have access to the most current and relevant evidenced-based guidelines for care. Finally, the model emphasizes the role of “Clinical Information Systems” to provide access to data, information, and knowledge needed to improve health. Effective and productive patient and provider interactions are the heart of the CCM and the key to improving outcomes. Over the last decade, the CCM has been implemented and evaluated in a variety of settings both in USA and in international studies. The CCM has proven to be a useful framework for patient empowerment, self-management support, and improving clinical and behavioral outcomes.
Our purpose of this CHIRA-JEEWA mission is to partly use this CCM with emerging e-health technologies and other feasible innovative concepts, to give a service which is more suitable to the Sri Lankan setup. This goal is consistent with the self-management support for chronic disease using technology tools suggested in both the Affordable Care Act (ACA) and the Health Information Technology for Economic and Clinical Health Act (HITECH Act) in USA. Also it is consistent with the existing Sri Lankan Government acts and health ministry empowerment.This mission is essentially a reflection and requirement of future health- care services.
1.8 Use of the Internet for Self-Management Support
In developed countries, the Internet serves as a conduit for self-management support, connecting providers and consumers to secure portals, health applications, social networks, and large databases. Roughly 80% of adults have sought health information on the Internet, including 62% of adults with a chronic illness; of those, 75% of the chronically ill surveyed stated their most recent Internet encounter affected decisions about the self-management of their condition . The Internet is also the vehicle used by many adults for access to social networking sites.
1.10 Social Networking or e-Health Communities:
Social networking or virtual communities are newer components of eHealth. A recent study reported in JAMA regarding the diabetes online community (DOC), “Tu-Diabetes”, found that the use of the social network augmented hypoglycemia surveillance among the members of that virtual community . To date, most research on the impact of social networks has been descriptive but there are a few studies that have shown improved health outcomes; no studies to date have shown adverse effects on consumers/patients ]. One randomized controlled trial (RCT) followed overweight and sedentary adults and found that the use of an online community helped maintain adherence to the program and that the participants had lower attrition from the study. In recent descriptive studies, virtual community members with diabetes and heart disease found that the environment was useful for asking questions, reporting personal experiences, and even supported eHealth literacy . Social networking may be an effective tool to encourage consumer empowerment and promote patient-centered care .
1.11 Telehealth:
One well-researched component of eHealth is in the area of telehealth, sometimes called telemedicine, which has been used extensively as an intervention across many aspects of health care. Telehealth (telecommunication, videoconferencing, remote monitoring, etc) can range from performing a detailed physical examination either synchronously or asynchronously, to using videoconferencing (audio/video technology) for the delivery of a class or training to individuals or groups in a remote setting.
The telehealth field is challenged with a clear definition. A recent study by Doarn et al 34. found there are seven United States government definitions for telemedicine. A standard definition of telehealth to facilitate the use and research eHealth tools is essential. To add strength to this movement, a federal telemedicine group was commissioned, FedTel, and legislation has recently been introduced to Congress to establish federal telehealth standards .
Telehealth has been especially effective in the management of diabetes. A recent systematic review evaluating 15 RCTs described that hemoglobin A1c (A1C), a laboratory examination that measures average blood glucose over the past 2-3 months, improved when telehealth interventions incorporated more elements of structured self-monitoring of blood glucose . Telehealth also lends itself to use by all members of the health care team. In a recent RCT, Tang et al 36 found that nurse-led, multi-disciplinary telehealth interventions were effective in improving A1C outcomes. In another nurse-led telehealth intervention designed for high-risk dialysis patients, the participants reported being more empowered and better able to provide needed self-management of illness . In a recent RCT, Young et al found that a telehealth nurse coaching model for people with diabetes produced higher self-efficacy scores in the control group than for those who received the usual care . Health care leaders, clinicians, and policymakers view telehealth as a powerful resource for improving health outcomes, health care quality, and to promote patient engagement.
1.12 Mobile Health
Mobile health (mHealth) components of eHealth span a broad spectrum of technologies. mHealth includes technology that is wireless, mobile, or wearable (eg, sensors, medication pumps, or wristbands that monitor physical activity). mHealth also includes thousands of health apps designed for mobile devices. The market for m-Health apps is anticipated to grow 25% per year with no foreseeable end in sight. mHealth is a “disruptive innovation” providing entrée to Internet-based health resources to groups who previously had barriers to these tools; 60% of Americans gain access to the Internet using a laptop, tablet computer, or mobile phone . Older adults, Hispanics, and African-Americans are adopting mobile technologies at a faster rate than the general population . Progress in the area of mobile phone text messaging has created a surge in using the tool for health self-management. Several recent studies and systematic reviews have reported modest health outcome improvement using text messaging as a targeted intervention .
Electronic Health Records/Personal Health Records (EHR/PHR):
The EHR is an electronic longitudinal record of care and patient information that may be shared across multiple health care settings . The tethered PHR, or patient portal, is a component of the EHR that communicates with the provider’s EHR or is integrated within the provider’s EHR and provides access to health records for patients/consumers and/or caregivers. The Markle Foundation defined the PHR as “an electronic application through which individuals can access, manage and share their health information, and that of others for whom they are authorized in a private, secure and confidential environment” (p. 14)(Markle Foundation, 2008)(Markle Foundation, 2008).
Health care leaders and policy makers highly recommend PHR use as a management tool for chronic illness . However, the PHR literature including systematic reviews related to use and health outcomes were inconclusive and the few RTCs conducted on PHR interventions failed to make the case for efficacy . While the scientific evidence does not demonstrate that using PHRs can improve health outcomes, the literature does support the impact on secondary outcomes related to self-management support . In an observational cohort study of 8705 subjects, Sarkar et al 54 found that patients with diabetes who use the PHR to refill their prescriptions had better medication adherence. In spite of some demonstration for the efficacy of PHRs in optimizing care, the PHR literature, including systematic reviews related to use and health outcomes, has been inconclusive .
With the national and international push to implement e-Health technologies into the current care environment, there is an opportunity to augment this well established CCM with integration of e-Health technology components. The CHIRA-JEEWA mission will going to demonstrate how adding e-Health components to this CCM may provide more self-management tools for the person with chronic illness.
2.Theoretical background of management science concepts
2.1 Definition of management
Management is the administration, organization and coordination of activities of an organization, whether it is a business, a not-for-profit organization, or government body in order to achieve defined objectives and goals. Management includes the activities of setting the strategy of an organization and coordinating the efforts of its employees (or of volunteers) to accomplish its objectives through the application of available resources, such as financial, natural, technological, and human resources.
2.2 Organizational environment
The organizational environment is the set of forces surrounding an organization that have the potential to affect the way it operates
and its access to scarce resources. The organization needs to properly understand the environment for effective management.
Scholars have divided these environmental factors into two main parts as,
A) Internal Environment
B) External Environment
A) Internal Environment: The internal environment consists of the organization's owners, board of directors, regulators, physical work environment and culture. In the internal environment include strength and weakness of an organization. Ex. Trade unions, Management, Current employees, Shareholders.
B) External Environment: In the external environment include opportunities and threats of an organization. In the external environment include legal, physical economic, technology, social, political, culture. The external environment consists of two layers. They are: 1) Task Environment: 2) General Environment.
1) Task Environment: Task environment is composed of the specific dimensions of the organization's surrounding that are very likely to influence of the organization. It also consists of five dimensions: Competitors, Customers, Employees, Strategic, Planners and suppliers.
2) General Environment: General environment is composed of the nonspecific elements of the organization's surrounding the might affect its activities. It consists of five dimensions: Economic, Technological, Sociocultural, Political-Legal and International.
2.3 Important / key points of management process
1.Division of work | Reduces the span of attention or effort for any one person or group. Develops practice and familiarity |
2. Authority | The right to give an order. Should not be considered without reference to responsibility |
3. Discipline | Outward marks of respect in accordance with formal or informal agreements between firm and its employees |
4. Unity of command | One man superior |
5. Unity of direction | One head and one plan for a group of activities with the same objective |
6. Subordination of individual interests to the general interest | The interests of one individual or one group should not prevail over the general good. This is a difficult area of management |
7. Remuneration | Pay should be fair to both the employee and the firm |
8. Centralization | Is always present to a greater or less extent, depending on the size of the company and quality of its managers |
9. Scalar chain | The line of authority from top to bottom of the organization |
10. Order | A place for everything and everything in its place; the right man in the right place |
11. Equity | A combination of kindliness and justice towards the employees |
12. Stability of tenure of personnel | Employees need to be given time to settle into their jobs, even though this may be a lengthy period in the case of the managers |
13. Initiative | Within the limits of authority and discipline, all levels of staff should be encouraged to show initiative |
14. Esprit de corps | Harmony is a great strength to an organization; teamwork should be encouraged |
Since the CJMS is a private business organization these business management concepts are widely used to achieve the goals of this mission. The most important concepts / principles used in this business model are summarized below.
2.3.1 Automatization of management process:
The organization is in a decision to use minimum number of human resources in the management process. Therefore computer software based automatization of clerical works, data (information) systems, financial (accounting) process & decision making process is a key feature of this business. This automatization ultimately results efficient & productive outcome.
2.3.2 Manageable workload for every employee/ stakeholder/ member:
Exhausting human resource during business operations is a major reason for failures & customer un-satisfaction. Since this is a medical service providing organization the quality of the service plays a major role for customer satisfaction. Therefore it always operates without exceeding the practical capacity of service providers (Ex. doctors, specialists, etc.) Also the mission is designed to recruit only eligible individuals as members who have the capacity to go ahead with terms & conditions of organization. This prevents joining customers who do not have the capacity to merge with this service. Because losing customers can damage the image of the business organization thus can leads to market un- popularity of brand name.
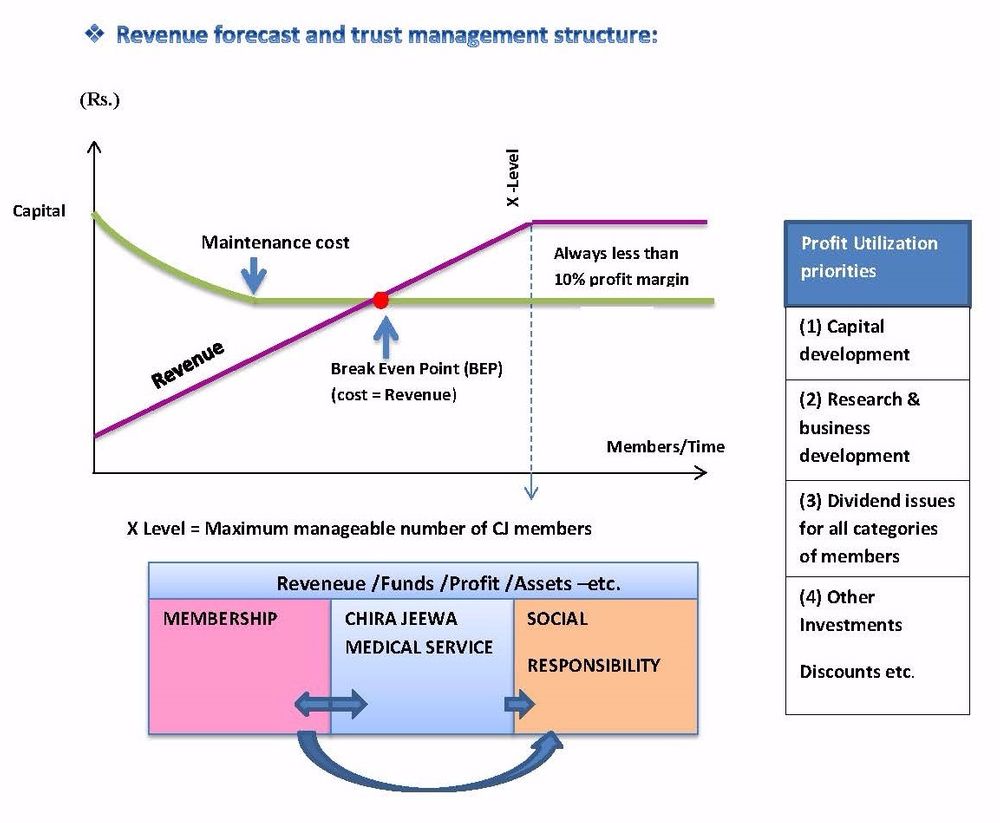
2.3.3 Reaching breakeven point (BEP) and making profits:
The diagram below demonstrates the theory behind this and its practical implementation in this business model
3.Theoretical background of I.T. concepts
- 100% privacy policy of information system and its large capacity is achieved by using cloud software/web development tool. This is password protected and has been backed up by two parallel URL domains. These two domains have different administrative accessibility with different passwords. So it will be impossible to hack personal information or attempt unauthorized access.
- Virtual nature of organization is achieved by mainly providing E-health services.
- A fast & convenient route of linking stakeholders (service providers & service receivers) in one interphase is achieved by maintaining an online information system.
3.1 About Cloud Computing
The term cloud computing first came about in 1960 and was used to express the notion that computing resources could someday be grouped together as a public utility. Today however, the term is used to describe a somewhat limited range of services, all of which adhere to some form of commonalities. When a company refers to ‘the cloud ‘or ‘a cloud’, they are generally referring to one of a number of technologies that are widely being used to replace the traditional server-infrastructure model. The cloud normally consists of a large number of servers; all linked to each other in such a way that they may be used by a number of parties, at the same time and are capable of reallocating resources to respond to demand at any given time. A classic application of this technology is a stock market monitoring service. Suppose we ran a service that monitors the New York Stock Exchange, the service would only ever be active during the hours that the exchange was trading, and where we to plot a graph of the server usage of such a service, it would not appear dissimilar to the parapets of an ancient castle. The application here is obvious, rather than paying for hundreds of servers to be running around the clock, the service could instead scale its infrastructure to cope with the load during peak periods, taking what Amazon.com refers to as ‘server instances’ offline whilst they’re not needed.
2.3.2 The Key Players
The theory behind cloud computing is at best subjective. There is no official standardized definition, which allows for a fair degree of ambiguity. There are however a number of large, incumbent suppliers in this relatively new market.
Perhaps the best known supplier of cloud computing solutions is Amazon, better known for its online book (etc.) store. The Amazon Web Services (AWS) are, arguably, some of the best, and cheapest, in the industry. If it’s net hosting that you’re in need of however, you’d be well advised to look into Microsoft’s offering and even then we’re barely scratching the surface. Other key players include IBM, Rack Space and even smaller hosts such as Media Temple (MT), offer similar, if not exactly comparable, solutions.
3.3 What’s so great about the cloud?
The main advantage to the cloud is its flexibility. The ability to expand an applications capacity to meet demand, without the need to purchase new hardware, it’s every server technician’s dream come true. There are however, other advantages. For applications that require large amounts of storage, the cloud model allows large quantities of data to be pushed to servers that are built to handle those large volumes of data, or if an application must process images or an infinite stream of data, servers that are ideally suited to that task can be assigned. The cloud allows for companies to not only scale the number, but also the type, of server that they use at any time. It’s here that the majority of savings are made when switching to the cloud.
3.4 Getting started with the cloud
Now we’ve considered what goes into the cloud and where it is a good idea. Let’s consider how we can best make a start using a cloud hosting service. The first task is to choose a cloud hosting provider, the de-facto standard seems to be the Amazon offering, AWS, which has been making waves across the web, from academic institutions to industry leading blogs and applications. Once we’ve settled on a service provider we need to look at just what we do and don’t want to be hosted there. Whilst the cloud is adaptable to almost any kind of service it does provide an additional level of complexity in some circumstances. Your personal blog, unless you get over half a million visitors a month, probably won’t benefit much from being moved to the cloud. A new service you’re developing to handle payments for a fortune 500 or an app for checking on car parking spaces in your local city however, are probably quite well suited to the ability of the cloud to quickly expand and shrink in line with demand. If you’re thinking of making the jump to the cloud, you’d do well to look into AWS as well as a few of its competitors. Once you’ve decided you’re going to make the switch it is strongly recommend gradually moving parts of a service over piece by piece, in order to minimize the effects of any problems that occur.
4.Theoretical background of co-operative concepts
4.1 Introduction:
The ancient Indian scripture rig Veda states; may you all have a common purpose may your hearts be in unison may you all be the same mind so that you can do work, efficiently well. The concept of co-operation is old as human society. It is the basis of domestic and social life. Science may points out the way to survival and happiness of all mankind through love and co-operation. Co-operation is derived from the Latin word “co-operari”, ‘co’ means “with” and ‘operari’ means “to work”. Hence co-operation means working together with others for a common purpose. Aristotle, a philosopher of ancient Greece, recognized the social nature of man when he said, “man is a social animal”. Man cannot lead a happy and contented life if he lives in isolation. Therefore, there is a great need for co-operation, which can be considered as the basic principle underlying human life. The word co- operation literally means working together or acts together.
Mclegan committee defines co-operation as “the theory of co-operation is very briefly, the isolated and powerless man can, by association with others and by moral development and mutual support obtain, in his own degree, the material advantage available to wealthy or powerful persons and whereby develop himself to the fullest extent of his natural abilities. By the union of forces, material advancement is secured and by united action self- reliance is fostered and it is from the inter-action of the influences that it is hoped to attain the effective realization of the higher and more prosperous standard of life which has been characterized as “better business”, “better farming” and “better living”. “Co-operative societies can help the transformation from capitalism to socialism and finally to communism”. – Lenin. The basic idea behind co-operation is “self-help and mutual help” and “mutual aid” and “each for all and all for each”.
The modern concept of co-operation is altogether different from the primitive one. “it denotes a special method of doing business” - different viewpoints of co-operation according to the sociologists co-operative movement is an instrument for establishing social harmony through the removal of class struggle. Economists are of the opinion that co-operative is a means of countering the exploitation of weaker sections by conferring on them a better economic status. In a legal sense, co-operation signifies special privileges and concessions conferred by law on its members. According to the socialist co-operative school, “co-operation is a weapon for the development of socialist thought and the realization of firms or households for business purpose and economic institution through which economic activity is conducted in the pursuit of economic objectives”
4.2 Features of co-operatives
1. It is an association of persons: a co-operative society comes into existence when a group of individuals join hand and form an association. 2. It is an enterprise or undertaking: co-operation lays stress on ethical standard and it is basically an enterprise. It is run by members themselves at their own cost and risk. 3. It is a voluntary association: an individual is free to join the society and resign from his membership of the society at his will and discretion. 4. It has service objectives: the main object of co-operative society is to serve its members rather than to earn profits. 5. It has democratic management: the co-operative society follows the cardinal principle of democracy i.e. One man one vote. The affairs are handled by the board of directors. The capital does not get any special treatment over human being in co-operation. 6. It is based on proportionality or equity: no discrimination among members is made on the grounds of religious faith, political ideology, and educational qualifications and so on. 7. It is with the norms of social justice: there is no class division among capitalists and working class in co-operation. 8. It is a socio-economic movement: a part of socio-economic movement the co-operative movement is viewed as a constituent part of the overall socio- economic movement of the country. 9. Proportionality or equality has a unique basis: the surplus is distributed not according to share taken but according to the proportion of business operation a member has effected with the society. 10. It is a universal movement: found in all countries of the world. 11. It is at the service of both the members and the community: every society stands for the economic upliftment of the members and the social, cultural and economic betterment of the local community.
4.3 Objectives of co-operation
Self-help made effective by organization is called Co-operative Society. The main objectives of co-operatives of co-operatives are: 1. Elimination of Middlemen. The First and foremost objective of co-operative society is to remove the middlemen in different fields, who take away the gains that should have gone to the real beneficiaries. 2. Raising economic status of the poor. The most basic aim of a co-operative society is to raise the standard of living of the poor. 3. Removal of the ills of capitalism. The basic cause of the ills of capitalism is the profit motive. This leads to exploitation, class struggle, economic inequality and unfair competition. These evils adversely affected the interest of workers and gave birth to co-operative movement. Therefore the aim of co- operation is to restrict the amount of profit and provide better service to its members. 4. Raising moral standards of its members. Co-operative movement wishes to direct human life towards goodness by raising their moral standard. 5. Increasing the prosperity of the whole community. . A co-operative society aims at bringing about the welfare of not a particular individual but of the whole community. 6. Abolition of Social Inequalities. The feeling of ‘high’ or ‘low’ among members of the community act as a cause of social tensions, the removal of which is the goal of the co-operative movement. 7. Political and religious neutrality. As far as possible, a co-operative remains aloof from political parties and religious groups. 8. Development of corporate life. A co-operative aims at providing a corporate life to the weaker sections of the community.
4.4 Benefits of co-operation
The benefits of co-operation are studied under four broad categories.
1. Economic benefits 2. Social and political benefits 3. Educational benefits
4. Ethical benefits.
The following are the economic benefits derived out of a co-operative institution. I. The substitution of profit incentive in business by that of service to the community. II. A more equitable distribution of wealth. III. A breaks up of monopolistic tendencies. . IV. Increase in purchasing power and real wages to individuals. V. Reduction in cost of distribution system by elimination of unnecessary middlemen. VI. The more accurate correlation of demand and supply. VII. Stabilization of employment. VIII. General improvement in employer, employee relationships. IX. Cheap marketing and processing of farm products at reasonable prices.
The important social benefits are as follows: I. To provide a unique education in democracy, responsibility and toleration. II. To train for political power. III. To evolve an industrial relationship among all. IV. To preserve a strong friendly or family spirit. V. To secure rational construction and unifying approaches to social and economic problems. VI. To prevent underemployment and unemployment. VII. To secure moral as well as physical satisfaction of pure quality, correct weight and fair dealings. VIII. To prevent exploitation of man by man.
Following are the important educational objectives or benefits of cooperation. I. The individuals lean by experience gained in practical work of co-operation. II. Co-operation also sponsors education. There are many co-operative schools and colleges formed to provide affordable education and also employment to educated unemployed youths. III. To train the people to take initiatives in organizing IV. To create experts.
Following are the important ethical and moral benefits of cooperation I. The policy of honesty is a necessity in co-operation. II. Cooperation returns money value for honesty and other virtues. III. The motto of co-operation is “each for all and all for each” IV. Co-operation aims at the production of fine human beings.
4.5 Seven co-operative principles
Cooperatives around the world generally operate according to the same core principles and values, adopted by the International Cooperative Alliance (ICA) in 1995. But in this CJMS business model these basic principles are strategically modified for the purpose of smooth flow of management process.
Principle 1: Voluntary and Open Membership
Principle 2: Democratic Member Control
Principle 3: Member's Economic Participation
Principle 4: Autonomy and Independence
Principle 5: Education, Training, and Information
Principle 6: Co-operation among Co-operatives
Principle 7: Concern for Community
4.6 INTERNATIONAL CO-OPEURATIVE ALLIANCE (ICA) PRINCIPLES
International Co-operative Alliance is an international body set up for the promotion of co-operative ideas and spreading the principles of co-operation around the world. Due to enormous changes taking place in Economic, Social and Political fronts, the International Co- operative Alliance (ICA) appointed a sub-committee in 1934 to take a fresh look at the co- operative principles. They evaluated the principles enunciated by Roach Dale, its relevance and observance in the present time and finally submitted its report in 1937. Based on the sub- committee report the ICA instead of formulating principles, they simply classified the Roach Dale Principles in to two- Essential and Non Essential in 1937. They are: 1. Open Membership 2. Democratic Control 3. Limited Interest on Share Capital Essential Principles 4. Patronage Dividend 5. Religious and Political Neutrality 6. Cash Trading 7. Promotion of Education Non Essential Principles 8. Selling Pure and Unadulterated goods 3.KARVE COMMITTEE ON CO-OPERATIVE PRINCIPLE. Again in 1960 due to the dynamic nature of the world, ICA appointed a commission in 1964. Five nations namely UK, USA, USSR, Germany and India were represented in the commission. Prof. D.G. Karve from India was the Chairman of the Commission and therefore, the Commission is popularly known as Karve Commission on Co-operative principles. The commission recommended the following principles in its report submitted in 1966. 1. Open and Voluntary Membership:-Membership of a Co-operative Society is open to all those who wish to join it. There is no discrimination on the grounds of caste, creed, religion, race, sex or politics. The only point to be remembered while giving membership is that his or her profession is not opposed to that of a co-operative society. For example a money lender is not admitted as a member of primary co- operative credit society. 2. Democratic Management:-The management of a Co-operative society should be done democratically. The ultimate responsibility of managing the entire society is vested with the School of Distance Education Co-Operative Theory & Practice Page 15 General Body. The main points to be taken care of in a democratic management are:- a) Each member has only one vote. b) Majority rules in all matters. c) Committee of management should always have the authority of members before they take any important step. According to the principle of democratic control, the Board of Management is an elected body, which controls the day to day affairs. 3. Limited Interest on Share Capital. As per the Co-operative Societi1es Act, 1969, interest on capital is restricted. For the purpose of collecting necessary amount of funds, the society is bound to pay interest. Whatever interest is paid, it should be on a limited scale. 4. Equitable Distribution of Surplus. Earning of profits is not the basic objective of a co- operative society. But this does not imply that co-operatives are run on no profit no loss basis, or they are managed with losses. The surplus of the society is disposed of as follows.. a. Provision is made for the development of the society. b. Provision is made for Common Services. c. Some of the surplus is distributed among the members on equitable basis. 5. Co-operative Education. The progress of the society depends to a greatest extent on how best its members can takes an active part in its affairs, which is possible only when the members are educated. Co-operative education includes: a. Education to members b. Education to office bearers; and c. Education of prospective members. 6. Co-operation among Co-operatives In order to best serve the interest of members all co-operative organizations should actively co-operate in every practical way with other co-operatives at Local, National and International levels. Such type of co-operation is necessary to acquire greater strength to face adverse conditions. 4.
4.7 CO-OPERATIVE PRINCIPLES BY ICA IN 1995.
The ICA Tokyo Congress held in 1992, initiated steps to review the current ICA Co- operative Principles of 1966 and make possible changes to prevent the erosion in values of co- operation. Based on the direction given to Dr. Ivan Mac Pherson (Canada), he reviewed the principles and submitted a report in 1994 which was approved by ICA General Assembly in Manchester in September 1995. This report contains seven principles:- The co-operative principles are guidelines by which co-operatives put their values into practice. 1. Voluntary and Open Membership Co-operatives are voluntary organisations, open to all persons able to use their services and willing to accept the responsibilities of membership, without gender, social, racial, political or religious discrimination. School of Distance Education Co-Operative Theory & Practice Page 16 2. Democratic Member Control Co-operatives are democratic organisations controlled by their members, who actively participate in setting their policies and making decisions. Men and women serving as elected representatives are accountable to the membership. In primary co-operatives members have equal voting rights (one member, one vote) and co-operatives at other levels are also organised in a democratic manner. 3. Member Economic Participation Members contribute equitably to, and democratically control, the capital of their co- operative. At least part of that capital is usually the common property of the co-operative. Members usually receive limited compensation, if any, on capital subscribed as a condition of membership. Members allocate surpluses for any or all of the following purposes: developing their co-operative, possibly by setting up reserves, part of which at least would be indivisible; benefiting members in proportion to their transactions with the co-operative; and supporting other activities approved by the membership. 4. Autonomy and Independence Co-operatives are autonomous, self-help organisations controlled by their members. If they enter into agreements with other organisations, including governments, or raise capital from external sources, they do so on terms that ensure democratic control by their members and maintain their co-operative autonomy. 5. Education, Training and Information Co-operatives provide education and training for their members, elected representatives, managers, and employees so they can contribute effectively to the development of their co- operatives. They inform the general public - particularly young people and opinion leaders - about the nature and benefits of co-operation. 6. Co-operation among Co-operatives Co-operatives serve their members most effectively and strengthen the co-operative movement by working together through local, national, regional and international structures. 7. Concern for Community Co-operatives work for the sustainable development of their communities through policies approved by their members. To conclude, that the above said principles are the important qualities that make co- operative institutions effective, distinct and valuable. The Government should provide a conducive environment for the co-operatives in which they may combine in their working co- operative values, socio-economic objects and competitive strength in the Globalized Era.
4.8 DIFFERENCE BETWEEN CAPITALISM AND CO-OPERATION.
In spite of these common features existing between capitalism and co- operation, there are a lot of differences between them on the following points. 1. In capitalism capital has a pivotal role to play in the business whereas in co-operation, it has a secondary role. 2. The capitalistic economy is dominated by profit motive whereas service is the motto of co- operatives. 3. In capitalism there is union of capital and in co-operatives there is union of persons. 4. Share capital determines the voting rights in capitalism whereas in co-operation, one man has one vote irrespective of their capital contribution. 5. Capital owns men in a capitalistic economy while in a co-operative society, men own capital. 6. In capitalistic system business tends to concentrate wealth in the hands of a few capitalist whereas in the co-operative system wealth is decentralized. 7. In capitalism there is cut throat competition whereas there is no such competition in 8. In capitalism the relationship is impersonal where as in co-operative business there exists a personal relationship between members and organization. 9. The evolution of capitalism is towards creation of monopolies, while evolution of cooperation is towards decentralization. 10. Capitalism encourages materialism whereas co-operations strive for development of cultural and spiritual values in individuals. 11. Capitalism maximizes the amount of profit or return of investment to shareholders. Co- operatives are formed for better economic service and improving the standard of living of its members.
4.9 CO-OPERATION V/S SOCIALISM INTRODUCTION:
Socialism is a system wherein all means of production and distribution is owned and controlled by the state. It is a socio economic system in which material means of production are owned by public authority or the community and operates not for profit but for the services of the community at large. Socialists are of different types and they are Marxism socialism or scientific socialism State socialism Guild socialism; and Evolutionary and revolutionary socialism The principles common to all socialist are substitution of collective ownership for private property in all instruments of production which permit exploitation of labour and the substitution of a central authority controlling production in place of the present competitive environment. But they differ in the views held as to how property should be held in common or as to how the distribution of services and goods should be carried out. In the words of KARL MARX “Society can be reformed only by the destruction of private property”. According to LENNIN “Mere growth of co-operation is identical with socialism”. FEATURES OF SOCIALISM The principles on which the majority of the socialists agree on may be listed as follows. 1. State alone has the power to organize and conduct production. 2. Nationalization of all the means or instruments of production ie., land, factories, mines, railways and their ownership to be transferred to the state. 3. Controlling Boards would be established in each industry and the state would pay wages fixed by such boards. 4. State would provide work for everyone. 5. The state itself would be capitalist, the landlord and the organizer of industry and thus interest and rent would disappear. 6. Remuneration for work would vary according to one’s ability and everybody is assured of an equal opportunity to rise in life, irrespective of rank. 7. The state would undertake production and distribution and pay costs of production and annex profits as well. Profits arising out of production would be spent by the state on education, medical relief, recreation and entertainment of the poor. 8. Private property in capital goods like residential house, furniture and fixtures and other consumer goods would be allowed. 9. Private ownership of means of production is prohibited. 10. Each individual is assured of fixed income. 11. The entire surplus or profits belongs to the state. 12. There is no class difference or class struggle; and 13. Balanced Economic development.
4.10 MERITS OF SOCIALISM.
The following are the advantages of socialistic pattern of society. School of Distance Education Co-Operative Theory & Practice Page 21 1. As the State runs the entire operations, considerable fund is accumulated with the State which can be used for amenities like education, medical facilities, free milk for children and for entertainments. 2. The productive resources are utilized in an effective manner. 3. Jobs neglected by people would be given to machinery and they would be free to pursue higher aims in life. 4. As equality of opportunity is afforded to all to rise to higher positions in life, considerable uplift of uplift of the masses is brought under a socialistic state.
4.11 SIMILARITIES BETWEEN CO-OPERATION AND SOCIALISM.
On the basis of the features of socialism we find that socialism and co-operation resemble each other in a variety of ways. They are: 1. Both aim at the abolition of class struggle, profit economy and poverty in the midst of plenty, which militate against the norms of a welfare state. 2. Both maintain economic equality and offer no opportunity for the development of glaring inequalities of income and wealth. 3. In both the forms, actions are directed towards the elimination of competitive forces and their substitution by the principles of co-operation. 4. Both aims at the welfare of the community and the promotion of social justice and progress. 5. Both oppose individualism and seek to replace it by collective ownership and collective action. 6. Both lay emphasis on distribution of wealth. 7. The aims of both are rendering of service rather than earning profit. 8. Both the systems are based on moral foundation and believe in human brotherhood. 9. Both the systems have a common origin; and 10. Both try for eliminating the evil effects of competition.
4.12 DIFFERENCE BETWEEN SOCIALISM AND CO-OPERATION.
The differences between the two are as follows. Basis of difference Socialism Cooperation System Socialism is a system of government which seeks to move towards its objectives by changing the prevalent economic order Co-operation is a system of thought which is compatible with all forms of economic and political systems. A better philosophy is enunciated within the system itself to help the common man to gain strength Type of Remedy Socialism is a political remedy for economic evils and it is effective through the active involvement of the Government Co-operation is a non-political alternative to the economic problems The state is supreme for it participates in and exercises The individual is supreme, he enjoys freedom of action. The School of Distance Education Co-Operative Theory & Practice Page 22 Supremacy control over production and distribution. The state interferes in all matters and the freedom cannot be exercised members direct the activities of the organization. Capital Socialism is against the idea of the accumulation of capital by individuals The co- operatives do not discourage accumulation of capital by its members. But in co- operation takes care to ensure that they are not controlled by it Role of the State Socialism operates under state domination, which is both the deciding authority and the directing agency. co-operatives seek to avoid state control Type of Property Socialism is associated with State Ownership. All the means are owned collectively by the community Co-operation is characterized by, the co-existence of private and collective ownership. Politics Politics in socialism, finds a top place Co-operation is free from politics or it is politically neutral Control Economy is controlled by the State Co-operative organizations are managed democratically Surplus In socialist economy the surplus goes to the state But in co-operatives it goes to the members on the basis of patronage dividend Object The objective of socialist economy is to protect the welfare of the people Co-operation the basic objective is service to members In spite of the difference, co-operation, in its broader sense, constitute an integral part of socialism. If co-operatives achieve the socialist objectives in bits, socialism extends its objectives to cover the whole country


Kind regards
CHIRA-JEEWA medical service.